")

Shoulder is a shallow ball and socket joint, it provides good mobility but becomes vulnerable to instability.

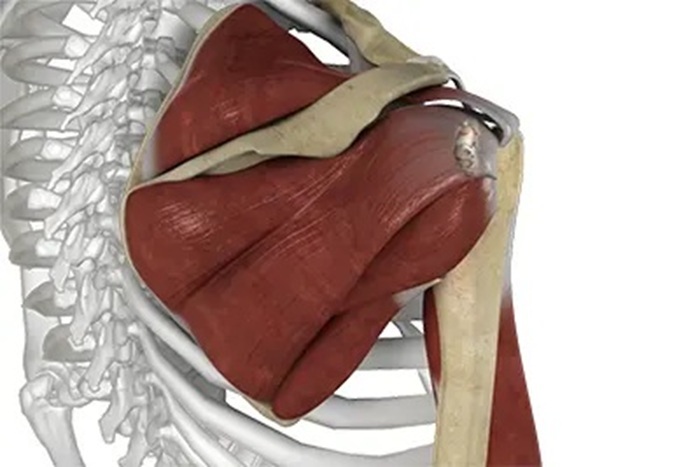
Shoulder basic functional anatomy
The shoulder joint is made up by four joints, including Sterno-clavicular joint, acromio-clavicular joint, gleno-humeral joint and scapula-thoracic joint. The first three joint are true synovial joint while scapulo-thoracic joint is only the articulation between scapula and thoracic wall without synovial structure.

Shoulder joint permits six direction of motion, including flexion, extension, abduction, adduction, internal and external rotation. The arm elevation is the combined motion at gleno-humeral joint and scapulo-thoracic joint, and it calls scapula- thoracic rhythm. The rhythm helps to move shoulder without causing impact inside shoulder joint.
Primary muscle groups around the shoulder include the muscles connecting torso and scapular ( Scapulothoracic ) , and the muscles supporting upper arm and scapular ( Rotator Cuff ). The trunk muscles help to move and stabilize the scapular on torso. While the rotator cuffs include supraspinatus, infraspinatus, subscapularis and teres minor, it helps stability and co-ordination of the upper arm on scapular.
Shoulder Pain Common Causes
- Sub-Acromial Impingement: sub-acromial space narrowing by tendonitis or bursitis
- Frozen Shoulder: known as Adhesive Capsulitis
- Long Head Biceps Tendonitis
- Acromioclavicular Joint Tearing / Separation
- Scapular Joint Dysfunction
- Rotator Cuff Tears
- Multidirectional Instability
Frozen Shoulder
Frozen Shoulder is known as adhesive capsulitis, it is characterised by gradually increase of shoulder pain and shoulder stiffness in both active and passive range of shoulder joint ( glenohumeral joint ). Early exercises are suggested until signs of acute inflammation, such as significant swelling and increased skin temperature, have already subsided. In very early stage, a more gentle active exercise, such as pendulum exercise, can be initiated to preserve shoulder joint flexibility. In later stage, gleunohumeral and scapulothoracic range of motion and strength exercises will also be emphasized daily training.
Early Acute Stage: Motions in shoulder are limited by severe shoulder pain. Shoulder exercises are only initiated by gentle pendulum motion, or even suggested to rest shoulder. Patients are advised to apply ice-pack to shoulder for pain relief.
Subacture Stage: Increased skin temperature and irritable shoulder pain being better is the cardinal sign for subacute stage. Patients are encouraged for moving their shoulder within pain-free range.
Recovery Stage: Exercises emphasize on regaining the range of motion. Strong stretching is suggested in this stage in order to regain the flexibility in shoulder joints.
Long head biceps tendonitis
Biceps is the muscle at the front side of upper arm, being responsible for bending elbow joint or turning forearm upwards. One of the attachments connecting to the scapular passes through the front side of upper arm, namely, long head tendon, gets irritation owning to chronic wear and tear. Patients might complain their painful shoulders when they try scratching their back. Therapist would confirm the physical diagnosis with specific examination, or even with MRI or ultra-sound report.
Acromioclavicular joint tearing / seperation
Normally there are a few ligaments connecting collarbone and shoulder blade bone. Owning to the sport injuries or contusion, tearing or rupturing of ligament would compromise the integrity of shoulder front side joint stability. Patients would complain collarbone joint pain whenever arm elevating.
How Traditional Chinese Medicine and Physiotherapy Help?
-
 Focused Extracorporeal Shockwaves
Focused Extracorporeal ShockwavesRelieve pain and promote healing from chronic tendinitis
-
 Acupuncture and dry needling
Acupuncture and dry needlingAcupuncture is safe and effectively treat chronic neck pain.1
-
 Cupping therapy
Cupping therapyReduce pain, and improve function and quality of life.2
-
 Manual therapy
Manual therapyRelease muscle tightness, improve joint alignment and function.
-
 Chinese Herbal Remedy
Chinese Herbal Remedy
Nature way of Pain Killer, and improve sleep quality.
-
 Exercise Therapy
Exercise TherapyPromote injured tissue healing, improve the function of the affected area.
FAQ:
Q1: Could you advise for the shoulder exercises?
A1: Exercises for shoulder generally includes strengthening and stretching. In acute stage, muscle tightening without moving joint ( Isometric exercises ) is encouraged in order to maintain muscle strength. In subacute and chronic stage, exercises focus on strengthening and stretching can help maintain good moving rhythm and posture of shoulder. Patients could make use of rubber tape or tube for their strengthening exercises.
Q2: Why there are some popping sound when moving shoulder?
A2: The joint moves with repeatable joint sound because of tendon thickening or problems from labral integrity. If joint sound starts after accident or injuries, it is better to take further diagnostic examination to rule out problems from labral rupturing.
Q3: How acupuncture may help shoulder joint pain?
A3: Acupuncture helps for relieving shoulder pain by pain gate control theory, or by promoting analgesic substance release in Central nervous system. Recently, researches also proposed that acupuncture might trigger release of serotonin and thus promoting anti-inflammatory effect.
Reference:
-
Cagnie, B., Struyf, F., Cools, A., Castelein, B., Danneels, L., & O’leary, S. (2014). The relevance of scapular dysfunction in Neck pain: A brief commentary. Journal of Orthopaedic & Sports Physical Therapy, 44(6), 435–439. https://doi.org/10.2519/jospt.2014.5038
- Giuseppe, L. U., Laura, R. A., Berton, A., Candela, V., Massaroni, C., Carnevale, A., Stelitano, G., Schena, E., Nazarian, A., DeAngelis, J., & Denaro, V. (2020). Scapular dyskinesis: From basic science to ultimate treatment. International Journal of Environmental Research and Public Health, 17(8), 2974. https://doi.org/10.3390/ijerph17082974
- Liu, S., Wang, Z., Su, Y., Qi, L., Yang, W., Fu, M., Jing, X., Wang, Y., & Ma, Q. (2021). A neuroanatomical basis for electroacupuncture to drive the vagal–adrenal axis. Nature, 598(7882), 641–645. https://doi.org/10.1038/s41586-021-04001-4
-
Melo, A. S. C., Moreira, J. S., Afreixo, V., Moreira-Gonçalves, D., Donato, H., Cruz, E. B., Vilas-Boas, J. P., & Sousa, A. S. P. (2024). Effectiveness of specific scapular therapeutic exercises in patients with shoulder pain: A systematic review with meta-analysis. JSES Reviews, Reports, and Techniques, 4(2), 161–174. https://doi.org/10.1016/j.xrrt.2023.12.006
-
Panagiotopoulos, A. C., & Crowther, I. M. (2019). Scapular Dyskinesia, the forgotten culprit of shoulder pain and how to rehabilitate. SICOT-J, 5, 29. https://doi.org/10.1051/sicotj/2019029
- Yin, C., Buchheit, T.E., Park J.J.. (2017, October). Acupuncture for chronic pain: an update and critical overview. Current Opinion in Anaesthesiology , 30(5), 583-592. doi:10.1097/ACO.0000000000000501.
Commonly seen related pain conditions